
Gambling is often reported to co-occur alongside other addictive and commercially determined behaviours, namely alcohol consumption and tobacco smoking.
Previous research in England has shown strong links between gambling risk, higher-risk drinking, and smoking, but much of this evidence is based on data collected before major changes in the gambling landscape such as the rapid growth of online gambling in recent years. With new data from the recently re-launched Gambling Survey for Great Britain, we took the opportunity to revisit these relationships using a large, nationally representative sample of almost 10,000 adults. This blog will touch on some of the key findings from our study published in the journal Addictive Behaviors on how risky drinking and smoking relate to risk or severity of gambling problems.
A “dose dependent” pattern
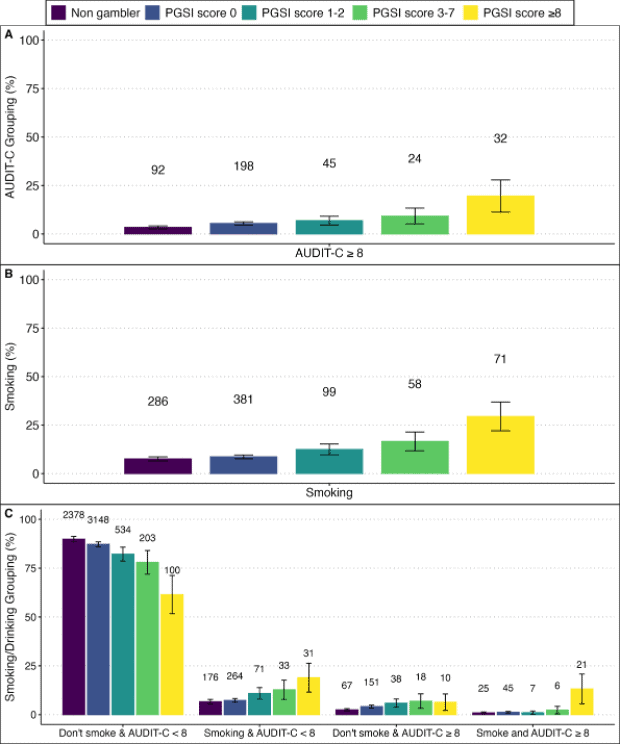
We found that levels of risky drinking (AUDIT-C score) increased in step with each of the four levels of gambling-related risk (according to the Problem Gambling Severity Index), from gambling without experiencing adverse consequences, to disordered gambling. Likewise, elements of loss of control of gambling (spending more than intending, ignoring spending limits or having a self-reported gambling “binge”), and tobacco smoking, followed a similar “dose dependent” pattern. Interestingly, we also found that those with the highest risk score (scores ≥8 on the PGSI; indicative of disordered gambling) experienced notable clustering of concurrent smoking and high-risk drinking (AUDIT-C ≥8).
These findings suggest that gambling harm, rather than simply gambling participation, is closely intertwined with other health risk behaviours.
Possible explanations
It is tempting to infer that in the case of alcohol consumption and gambling, increases in one behaviour causes an increase in the other. Increased alcohol consumption could reduce self-control and risk aversion and increase enjoyment of gambling, and certain gambling environments could drive risky alcohol consumption through directly supplying it (as in bars with gambling facilities or in casinos), or by promoting or establishing norms around alcohol consumption and gambling.
Unfortunately, the data in our study are not collected in a way that can help us confirm these explanations, as plausible as they might be. Rather than one behaviour causing an increase in the other, it is likely that this pattern is also down to gambling and alcohol consumption having common causes that determine changes in both, such as mental health problems or underlying social conditions. Nonetheless, further research could examine the social and environmental context of the activity (e.g. in a pub/bar setting) or the characteristics and gameplay of the activity itself (e.g. continuous, fast-paced and instant win) that could interact with the drug-specific behaviours and effects of alcohol consumption.
Policy, intervention and research: a cross-behavioural lens
Our findings should reinforce the adoption of a cross-behavioural approach to public health, especially in the context of gambling and alcohol use. This involves greater sensitivity to how the behaviours relate to and reinforce one another when delivering individual- and population-level interventions. For instance, a joined-up approach to treatment has the potential to improve outcomes and reduce relapse risk for those experiencing the greatest level of harm. In terms of policy, national campaigns could highlight the additive risks of concurrent behaviours, and proposed advertising restrictions on gambling or alcohol should not be considered in isolation but act in concert to reduce exposure in contexts such as live sporting events where both alcohol and gambling promotions are commonplace.
Gambling-related harm is part of a broader constellation of risk behaviours that are driven by shared structural and neurobiological factors. Policies and interventions that situate gambling within this wider framework of addiction and harm have the potential to deliver population health benefits.
Written by Dr Loren Kock, Senior Research Fellow, Department of Behavioural Science and Health, Institute of Epidemiology and Health Care, University College London (UCL).
All IAS Blogposts are published with the permission of the author. The views expressed are solely the author’s own and do not necessarily represent the views of the Institute of Alcohol Studies.