

In this month’s alert
The missing policies in the UK’s 10-Year Health Plan – podcast feature
This month’s episode of the Alcohol Alert Podcast is a special cross-post from The Alcohol Debate Podcast, hosted by alcohol-freedom coach Tabbin Almond. In this episode, Tabbin is joined by Jem Roberts, Head of External Affairs at the Institute of Alcohol Studies, for a wide-ranging discussion on alcohol policy in the UK and Ireland.
From Ireland’s world-first alcohol labelling law and its recent delays, to the UK Government’s 10-Year Health Plan and the omission of minimum unit pricing, Jem explains how political choices – and industry lobbying – shape the nation’s response to alcohol harm.
Pricing policies have a really quick effect on saving lives. So if you want to be coming into the next general election showing tangible results from your policies, they’re pretty good policies to introduce.
Subscribe to Tabbin’s podcast on Apple, Spotify, or most other podcast platforms.
Drink drive limit could be reduced in England and Wales
A new road safety strategy set to be published in the autumn is expected to reduce the drink driving limit in England and Wales to match Scotland’s limit.
England and Wales have the highest limits in Europe, at 50mg of alcohol per 100ml of blood – no other country has a limit this high. Scotland reduced the limit to 50mg in 2014 and Northern Ireland have passed legislation to lower the limit to 50mg but are yet to implement this change.
Deaths and injuries from drink driving fell significantly from 1980 to 2010, plateaued for 10 years before starting to creep up in the last few years. In 2023 there were 260 deaths – a 13% increase since 2011 – and almost 2,000 casualties. 16% of all road traffic deaths are due to drink driving.
IAS sent a letter to the Transport Secretary in support of the decision, highlighting other recommendations that should be brought in alongside a reduction in the limit, including increased enforcement through breath testing, specialist rehabilitation courses for those with mental health and alcohol problems, and improving the High Risk Offender Scheme.
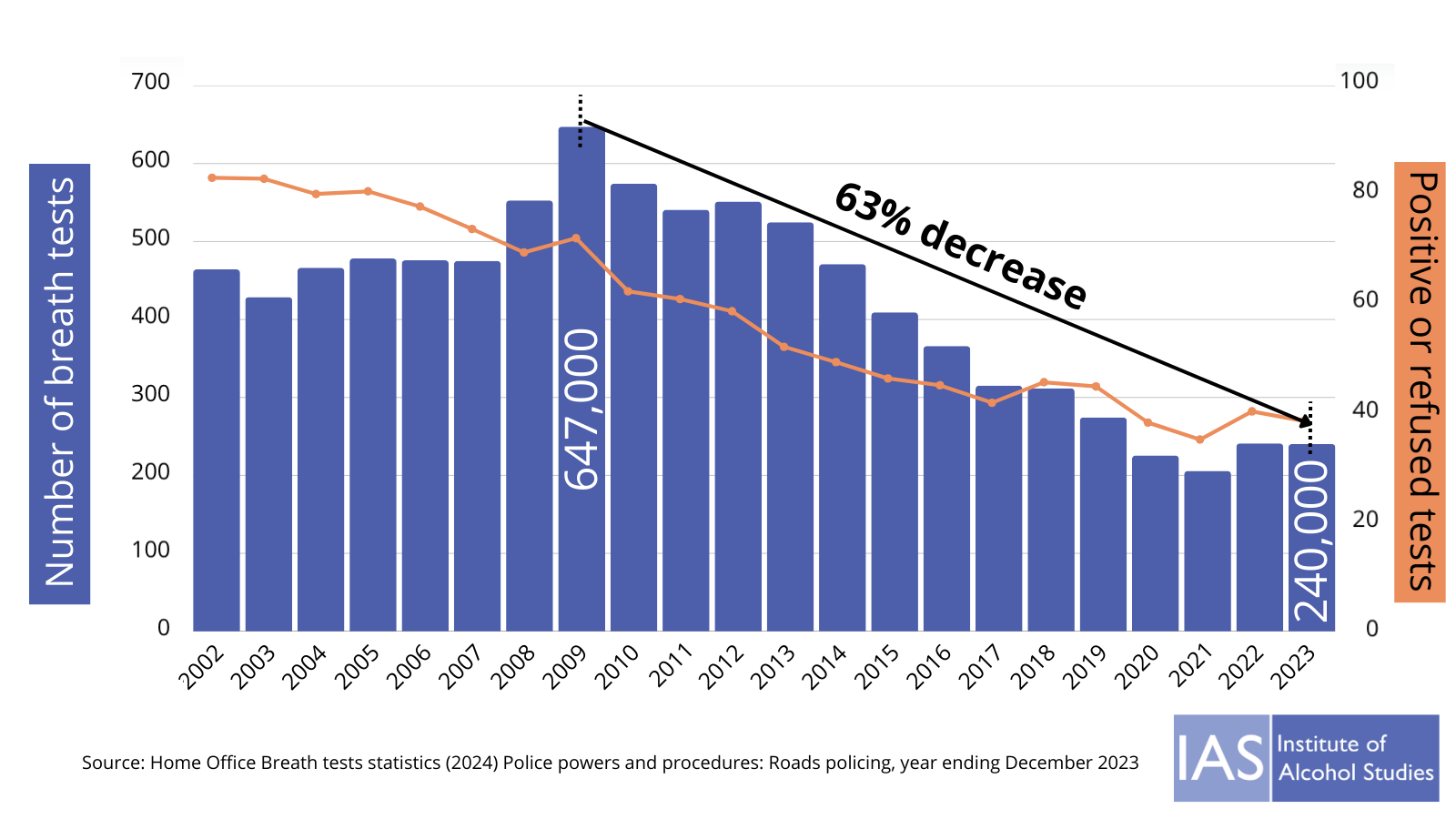
In a recent IAS blog, IAS’s Jem Roberts and Dr Katherine Severi laid out the evidence for lowering the limit and tackled arguments made against reducing it. One of the main arguments that will continue to be cited in the coming months is that studies have found reducing the limit in Scotland didn’t save lives. However, two of the researchers that found this explained to the i paper that greater enforcement and public transport options are crucial for reductions to work. Breath testing levels have plummeted in recent years, falling from a peak of 647,000 in 2009 to only 240,000 in 2023, yet the proportion of tests that were positive or refused has risen from 10–12% in the mid-2010s to around 16-17% in recent years.
Public awareness campaigns are also important, with a recent poll finding that 82% of people are unable to correctly identify the limit, despite half saying they understand it.
The Morning Advertiser highlighted the diverse opinion among publicans, with many supporting the decision. The Scottish Licensed Trade Association explained that there were many more important issues facing the pub industry, and that if England and Wales reduce the limit: “There will be some impact, but going forward I think that should recover pretty quickly.” Another said that: “In fact, a total ban would be easier to implement and understand.”
The government’s plans are “not sufficient to address the scale and complexity of alcohol harm”

In early August, the Alcohol Health Alliance – alongside over 30 leading experts in health, treatment, and policy – wrote to Secretary of State for Health and Social Care Wes Streeting to call for an urgent and ambitious strategy to address rising alcohol harm, after key policies on alcohol were removed from the final version of the NHS 10-Year Plan.
While the group welcomed measures such as alcohol labelling and community-led initiatives included in the 10-year plan, they argued that these are not sufficient to address the scale and complexity of alcohol harm.
The signatories called for policies that are proven to reduce harm and health inequalities, including minimum unit pricing, an alcohol duty escalator, and better treatment pathways.
The letter stressed that “alcohol is not just the problem of a few”, with 30% of adults engaging in “risky drinking”, almost one in 25 of all new cancers linked to alcohol, and over one million hospital admissions every year.
A Department of Health and Social Care spokesperson said it will continue to consider the most effective interventions to reduce alcohol harms, and that:
As we shift from sickness to prevention through our 10-Year Health Plan, we will make it mandatory for alcoholic drinks to display health warnings and nutritional information. To improve drug and alcohol treatment services and recovery support in England, the Government has also provided an additional £310 million in 2025/26, on top of the public health grant.
Licensing taskforce: Government responds, but health still missing

In April, we reported that the government’s new Licensing Policy Taskforce – co-chaired by Gareth Thomas MP (Department for Business and Trade) and Greene King Chief Executive Nick Mackenzie – contained no health representatives. The group’s remit was to recommend reforms to modernise licensing and support the growth of the hospitality and night-time economy.
The taskforce published a report with recommendations in late July and on the same day the government published its response. In his foreword, Minister Gareth Thomas acknowledged that one in four pubs have closed since the Licensing Act was introduced over 20 years ago. He stressed the importance of pubs and other licensed venues as regulated spaces, warning that growth in drinking in unregulated settings poses risks to both safety and health.
The government says it accepts the majority of the taskforce’s recommendations, subject to further consultation. These include:
- Developing a National Licensing Policy Framework, to guide local licensing authorities while preserving local discretion.
- Introducing an ‘amnesty’ to modernise and streamline licences.
- Ending the requirement for printed statutory notices for alcohol licence applications.
- Simplifying licensing processes for outdoor areas.
- Reviewing the Temporary Event Notice (TENs) system, including raising the maximum.
- Requiring time-limited reviews of blanket licensing policies, such as core hours.
While these measures are welcomed by industry as reducing red tape and helping venues adapt, concerns remain that health has again been left off the agenda. Neither the Department of Health and Social Care nor public health representatives are engaged in shaping reforms.
A public health perspective
If the government is serious about tackling unregulated drinking, licensing reform could be an opportunity to bolster public health protections rather than sideline them, particularly by introducing a public health licensing objective and significantly increasing the price of alcohol in the off-trade via minimum unit pricing and raising alcohol duty.
The government’s response reflects industry priorities for growth and flexibility. But without embedding health into the licensing system, there is a risk that reforms weaken protections at a time when alcohol-related harm remains high.
Transparency concerns
Another interesting angle highlighted by the Camden New Journal is the potential impact of removing printed statutory notices from the licensing system. Local newspapers often rely on income from carrying these notices, and their removal may reduce transparency and public awareness of licensing decisions. This could leave communities “in the dark” about new licences in their area.
A consultation on the proposals will be launched in due course.
Health experts call on Education Secretary to ban school materials backed by alcohol, gambling, and junk food firms

58 organisations – including academics, health charities and advocacy groups – have written to the Education Secretary, urging the government to protect children from misleading classroom materials funded by industries whose products harm health.
The letter, reported by The Guardian, warns that companies are providing schools with resources about the very harms caused by their own products. Evidence shows such materials routinely misrepresent science, normalise risky behaviours, and shift responsibility onto individuals, including children.
Chris van Tulleken, Professor of Infectious Disease and Global Health at University College London said:
We wouldn’t let Big Tobacco teach children about smoking. So why are we allowing the alcohol, gambling, and junk food industries into classrooms? Allowing these industries into schools distorts learning and helps industry establish the next generation of customers.
The signatories argue that removing industry influence would support the government’s health mission to prevent ill health and reduce inequalities.
Recent investigations have revealed how far commercial interests reach into UK schools. Examples include:
- Alcohol: Drinkaware materials encouraged students to reflect on whether “drinking alcohol makes you happy,” alongside cheerful images of young people drinking. Resources from the Alcohol Education Trust (now the Talk About Trust) and Diageo’s Smashed programme contain misinformation about the links between alcohol and cancer, and Smashed materials misinform about drinking during pregnancy.
- Gambling: Industry-funded charities have supplied lessons teaching students how to use betting slips and promoting “responsible gambling” while downplaying marketing’s role and exaggerating programme effectiveness.
- Food: Multinationals such as McDonald’s, PepsiCo and Kellogg’s have distributed branded lesson plans and sponsored breakfast clubs, giving companies subtle but pervasive access to children.
Dr May van Schalkwyk, Research Fellow at the University of Edinburgh, said:
The evidence is clear. Industries whose products are undermining the health and wellbeing of children and young people fund harmful youth education programmes as part of their corporate strategies. Urgent action is needed to prevent this form of influence and conflicts of interest.
The letter calls for clear government guidance – as introduced in Ireland – requiring schools to avoid materials funded by harmful industries. Educational content, it argues, should always be developed and delivered independently of vested interests.
Alcohol giant Diageo defended its Smashed initiative, claiming it had educated “hundreds of thousands of young people” and was valued by teachers.
The Department for Education responded that schools are responsible for choosing their own resources and ensuring they are suitable and impartial. Updated RSHE guidance warns schools to be cautious about using materials from organisations with “a broader interest in promoting harmful products.”
But health experts say the government’s hands-off approach is inadequate. A major problem is the expectation that teachers can identify and navigate industry tactics, even when they are hidden behind charities. Educators should not be left to police conflicts of interest. Instead, the government must provide safeguards to ensure all classroom materials are independent, trustworthy, and free from commercial influence.
In related news, the family of a woman who died from suspected methanol poisoning while travelling in Southeast Asia have succeeded in their campaign for compulsory education about the issue in schools. The government said it has now updated the curriculum on increasing personal safety while drinking alcohol, including how to avoid poisoning from potentially fatal substances, such as methanol.
Health advocates warn UN NCD Declaration weakened amid industry pressure

The UN’s upcoming High-Level Meeting on non-communicable diseases (NCDs) in September is drawing criticism from public health advocates, who say the latest draft political declaration has been weakened under pressure from “big tobacco, alcohol, junk food, and fossil fuel” industries.
Civil society groups argue that the changes dilute commitments to effective interventions, including taxes on unhealthy products, marketing restrictions, and mandatory labelling.
Alison Cox, director of policy and advocacy at the NCD Alliance, said:
It looks like health-harming industry fingerprints are all over this. At a time of fiscal pressures, shrinking global health funding, and increased emphasis on domestic resource mobilisation, health taxes are a golden opportunity to both generate revenue and reduce the burden of NCDs and associated healthcare costs. Yet as it stands, the declaration’s text contains weaker language around taxes and lets industry off the hook, prioritising profits over public health.
Analyses show that the revised declaration has replaced strong action-oriented language such as “implement” and “enact” with softer terms like “consider” and “encourage.”
Measures previously included in the Zero Draft to reduce alcohol harm – covering marketing, availability, and drink-driving laws – have largely been removed. Movendi International described this as a “textbook case of policy capture,” warning that it risks making the declaration meaningless while ignoring alcohol’s leading role in death and disability among 15–49-year-olds.
The draft also scales back commitments on sugary drinks, tobacco packaging, and food labelling. South African public health lawyer Safura Abdool Karim cautioned:
It’s supposed to be the bold agenda we aspire to… not a humble, conservative set of asks.
Civil society groups are urging negotiators to resist last-minute compromises that prioritise commercial interests over public health, restore evidence-based measures, and retain time-bound targets. Without these steps, advocates warn the declaration may fail to curb the growing global burden of NCDs.
New study reveals January drinking dip is only temporary
A new study has found that while January sees clear drops in alcohol sales and a rise in alcohol-free or low-alcohol (“no/lo”) alternatives, these changes are not sustained in the long term.
Researchers from the University of Sheffield and partners analysed population-level sales data from bars and shops across Great Britain. They found that standard alcoholic drink sales were consistently lower in January, while no/lo drinks peaked during the same month.
The authors note:
There was evidence of a short-term seasonal effect of January such that sales of standard alcoholic drinks decreased and sales of no/lo drinks increased overall during this period.
However, the present study found no strong evidence that population-level reductions in drinking during January has a long-term impact on alcohol consumption trends.
The findings suggest that campaigns like Dry January encourage temporary behaviour change, but more support may be needed to achieve lasting reductions in drinking.
A third of young social media users saw alcohol posts by businesses in last month
A new survey and report by Cancer Research UK have shown the prevalence of unhealthy commodity content targeting young people on social media.
The Digital influence report looks at the awareness of and interaction with online marketing for cigarettes, vapes, HFSS products, and alcohol among 11-21 year olds.
Regarding alcohol:
- 36% of young social media users reported seeing posts relating to alcohol by businesses in the past month
- 38% saw posts by influencers
- Over 18s who already drank alcohol said it could influence them to want to drink.
Views on potential policy options for social media marketing varied significantly between the product groups. On alcohol, the survey found that over half of young people supported making the social media accounts of alcohol business private and almost half felt that if accounts couldn’t be made private, alcohol businesses shouldn’t be allowed to have an account. Almost half of young people disagreed that it was OK for influencers to promote alcohol on social media.
Most young people believed that the responsibility for preventing alcohol promotions to people under the age of 18 lies with social media companies, alcohol companies, and governments.
Ultra-brief alcohol intervention shows no benefit in trial
A major trial in Japan has found that an ultra-brief alcohol intervention delivered by doctors in under one minute was no more effective than simple screening at reducing hazardous drinking. The study, involving over 1,100 primary care patients, showed no significant difference in alcohol consumption between the intervention and control groups after 24 weeks.
Commenting on the findings, experts noted that:
the early promise of alcohol screening and brief intervention has not been borne out in subsequent trials of real world effectiveness.
They suggest greater value may lie in identifying higher-risk patients for specialist treatment.
Hospitality sector faces job losses and market shifts
The UK hospitality sector has seen a significant share of recent job losses, with restaurants, pubs, bars, and hotels accounting for around 53% of roles cut since last October, according to UKHospitality analysis of ONS data. This equates to roughly 89,000 positions.
Rising operational costs – including business rates, VAT, National Insurance contributions, and an increase in the minimum wage – have been cited as contributing factors, alongside wider economic pressures such as inflation and reduced consumer spending.
Data from the Office for National Statistics show that overall payrolled employees in the UK fell by 149,000 between June 2024 and June 2025. Surveys suggest that many hospitality businesses have responded by reducing staff, shortening opening hours, or raising prices.
Reports indicate nearly eight in ten pubs and restaurants have increased prices in response to higher costs, and over half have reduced staff numbers since April.
The sector is also undergoing structural changes. Managed, branded, and franchised operators – representing just over a quarter of total pub sites – are projected to account for more than half of the market’s value by the end of 2025. Independent pubs, meanwhile, face ongoing challenges, including closures averaging eight per week so far this year. Yet market analysts forecast steady growth overall, with diversification into areas such as events, co-working spaces, and accommodation expected to support recovery.
Alcohol Toolkit Study: update
The monthly data collected is from English households and began in March 2014. Each month involves a new representative sample of approximately 1,700 adults aged 16 and over.
See more data on the project website here.
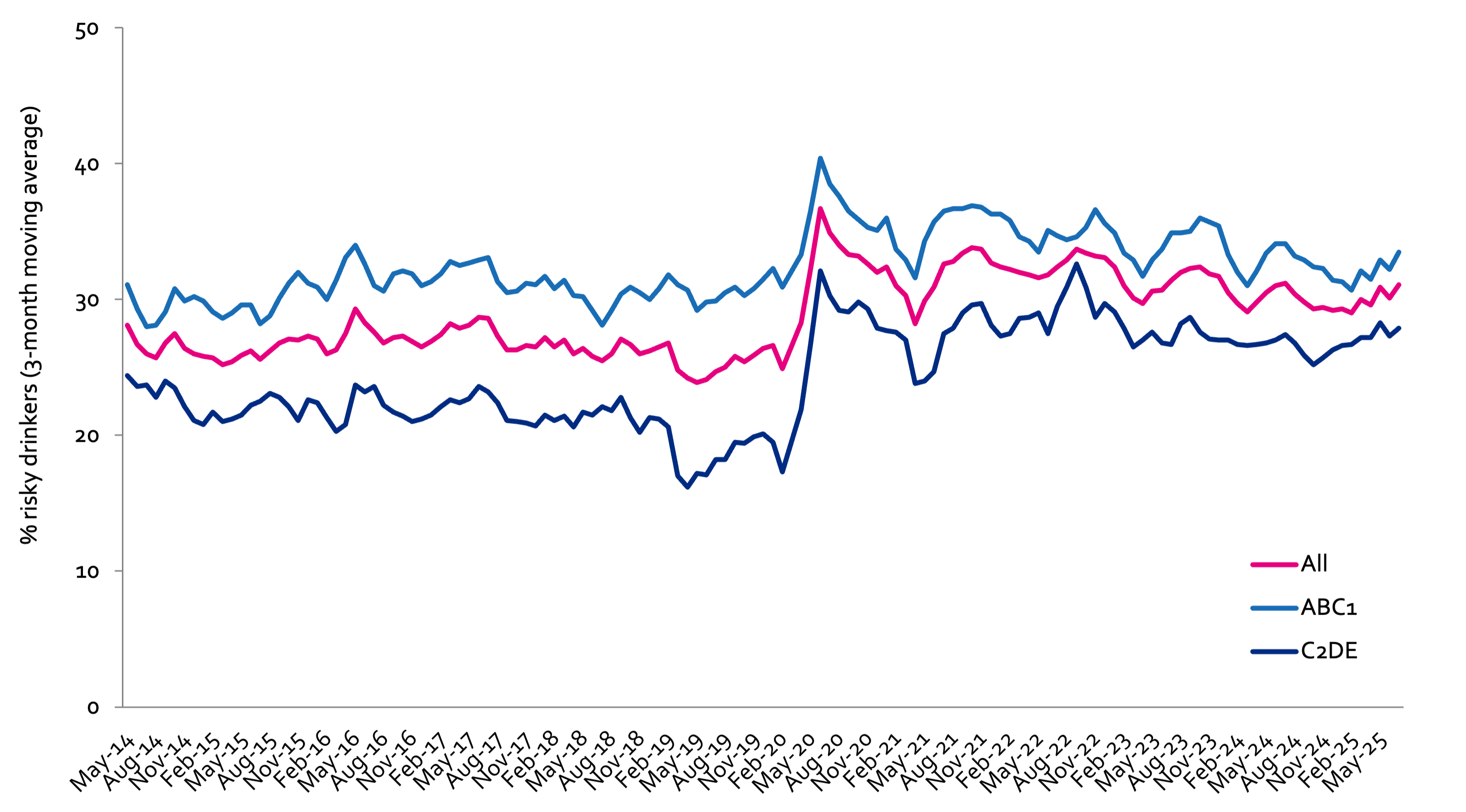
Prevalence of increasing and higher risk drinking (AUDIT-C)
Increasing and higher risk drinking defined as those scoring >4 AUDIT-C. A-C1: Professional to clerical occupation C2-E: Manual occupation
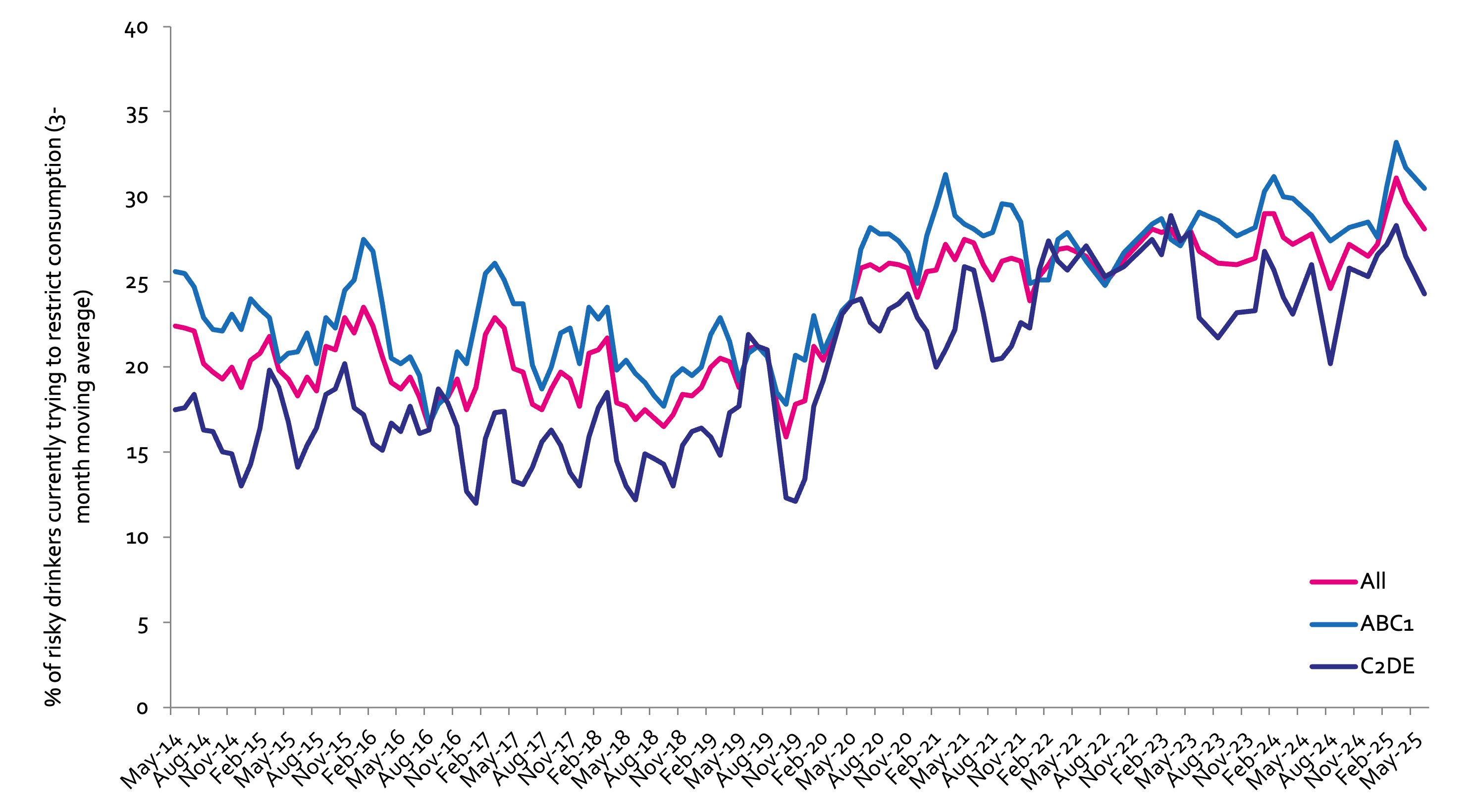
Currently trying to restrict consumption
A-C1: Professional to clerical occupation C2-E: Manual occupation; Question: Are you currently trying to restrict your alcohol consumption e.g. by drinking less, choosing lower strength alcohol or using smaller glasses? Are you currently trying to restrict your alcohol consumption e.g. by drinking less, choosing lower strength alcohol or using smaller glasses?
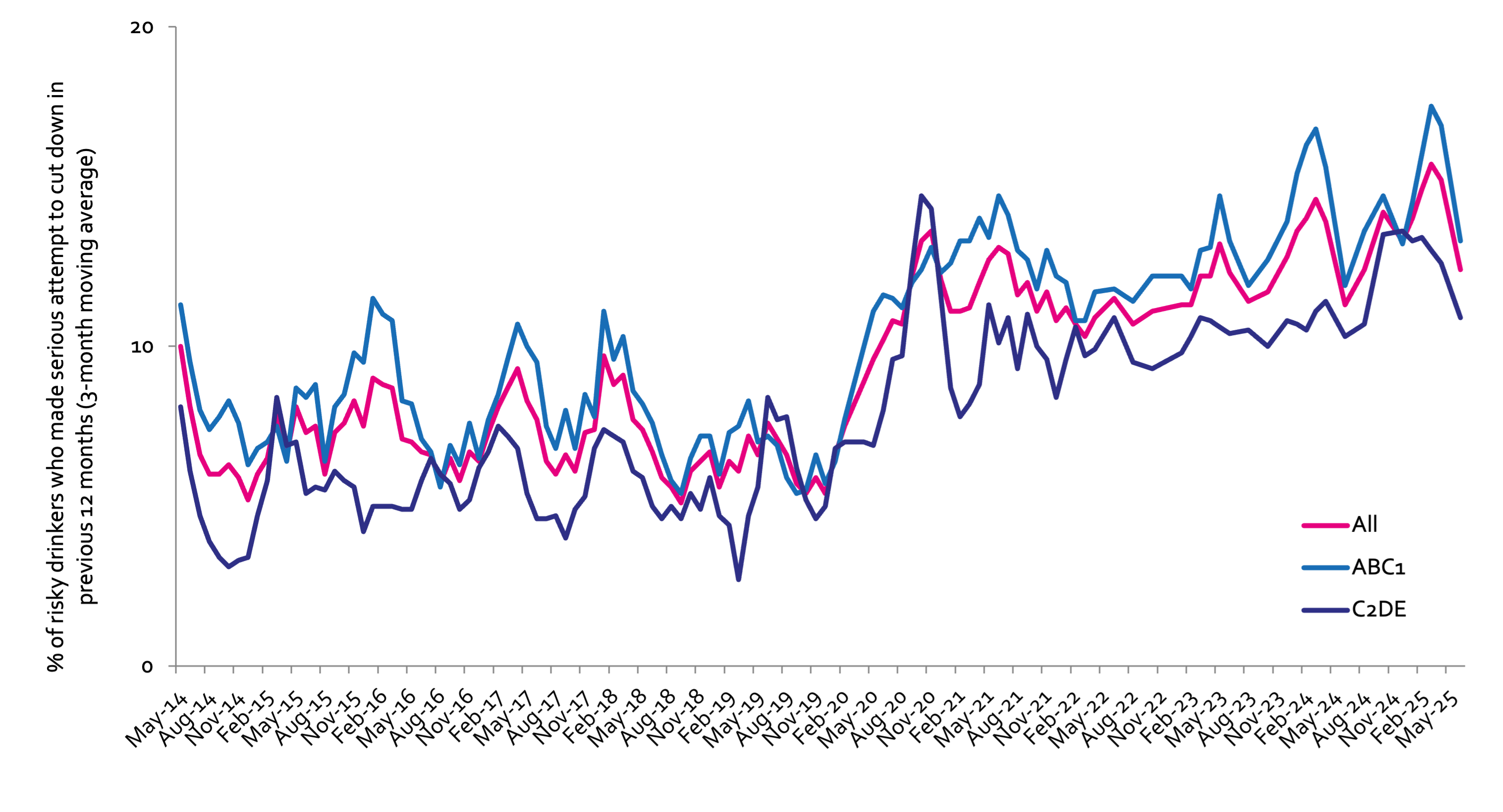
Serious past-year attempts to cut down or stop
Question 1: How many attempts to restrict your alcohol consumption have you made in the last 12 months (e.g. by drinking less, choosing lower strength alcohol or using smaller glasses)? Please include all attempts you have made in the last 12 months, whether or not they were successful, AND any attempt that you are currently making. Q2: During your most recent attempt to restrict your alcohol consumption, was it a serious attempt to cut down on your drinking permanently? A-C1: Professional to clerical occupation C2-E: Manual occupation
Podcast
Our monthly podcast features interviews with experts from across the sector.
Hooked by design: how social media fuels alcohol harm
Professor Nicholas Carah –
The University of Queensland